THE SHOULDER: A COMPLEX JOINT
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Human anatomy can sometimes seem complex to those who are not familiar with it. There is even one joint so complex, that even health specialists may have difficulty understanding it completely: the shoulder. Given the multitude of movements it must allow and the large number of muscles that are required to ensure them, it is actually not surprising that a level of complexity is required. I therefore propose to explain to you today, to the best of my ability, the anatomical and pathological bases of the shoulder.
The shoulder: what is its composition?
Let's start by making one thing clear: the shoulder is not just a joint, but is composed of three joints and a pseudo-articulation. First, we have the glenohumeral joint, composed of the scapula and the humerus; it allows the majority of the shoulder's articular amplitude. There is also the acromioclavicular joint which involves movement between the acromion, which is a bony landmark of the scapula and the clavicle, and thirdly, the joint between the clavicle and the sternum. These two joints, although limited in the motion they govern, are crucial for a full and healthy range of motion. The pseudo-articulation mentioned above is the scapulothoracic. It is said to be pseudo, because it is not composed of two bones connected together by ligaments or by bony facets, but by muscles. Nevertheless, many movements are only possible by a movement of the scapula in relation to the thoracic bone.
How does it work?
The movements of the shoulder are composed of several axes that are divided into two families: the movements of the humerus and the movements of the scapula. In the first family, there is the abduction/adduction axis, which raises the arm to the side and brings it closer to the center of the body, the flexion/extension axis, which propels the arm forward and backward, and the internal/external rotation axis, which rotates the anterior aspect of the arm toward the center of the body or toward the side. In the second family, the three axes of movement are elevation/lowering, which translates the scapula up or down, abduction/adduction, which moves the scapulae to the side or closer together, and external/internal ringing, which is a tilting of the tip of the bone to the lateral top or a return to its anatomical position.
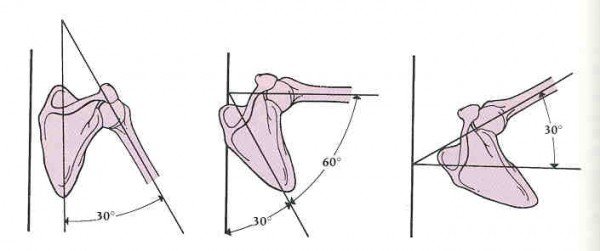
These two families of movement merge to create the movements as we perform them on a daily basis working together. An example of this is the abduction of the arm. This is sometimes referred to as the scapulo-humeral rhythm in abduction, which is the coordination of movement between the different joints involved. As you can see, the first thirty degrees of abduction are strictly performed at the glenohumeral level, then the scapula moves, and finally the last ten degrees of amplitude are possible thanks to the sternoclavicular joint.
As mentioned above, scapulothoracic stabilization is provided only by muscles and the amount of movement requires a large number of muscles. The rhomboids connecting vertebrae C7-T5 to the medial border of the scapula secure the scapula primarily in adduction. Predictably, the scapula elevator, connecting C1-C4 to the upper tip of the scapula performs elevation. The trapezius, on the other hand, covering a large area from the occiput to the tenth dorsal vertebra to the clavicle, the acromion and the spine of the scapula, exert several forces on the scapula, always in adduction, and sometimes in elevation, sometimes in lowering, or even in internal or external ringing, depending on the muscle bundle in action. Working in the opposite direction to all these, the serratus anterior, connecting the underside of the scapula to the first eight ribs, acts in abduction of the scapula.
The glenohumeral movement is performed by even more prominent muscles. The deltoid, connecting the clavicle and the spine of the scapula to the humerus, performs a great deal of abduction and flexion or extension of the shoulder depending on the muscle fiber in question. In front, the pectoralis major, originating at the sternum, the first six ribs and the clavicle and ending at the bicipital groove of the humerus, forces in flexion, abduction and internal rotation. The greater dorsalis, on the other hand, forces in adduction, extension and internal rotation, joining its insertion at the bicipital groove and its origin at the T7-L5 vertebrae, the sacrum and the iliac crest. What many people forget is that glenohumeral stability is managed by the muscle group known as the rotator cuff, which includes the supraspinatus, subspinatus, subscapularis and pudendal muscles. These four muscles allow a solid sheathing, especially in rotation, while the larger muscles confer mobility.
It is common for the scapulohumeral rhythm to be changed by muscle contractures and poor movement habits. One such change is that the glenohumeral joint is not strong and mobile enough to do its share of work, requiring additional and more frequent scapular movement. In someone who spends a lot of time sitting at work, this can translate into neck and wider postural problems that are quite complex. So making sure you have good scapular mobility and shoulder movement patterns is a good habit to get into.
Also, you may have noticed that a lot of muscles pass through the subacromial region to move the humerus. This subacromial space is indeed very small and the slightest inflammation can have great repercussions. Shoulder tendinitis is quite common and, being the most frequent, tendinitis of the biceps brachii and supraspinatus, both of which pass through this space, can lead to complications. If left to their own devices, they can degenerate into bursitis, spreading the inflammation to this structure that serves as their mechanical pulley, which in turn can inflame the capsule that encloses the joint and degenerate into capsulitis. Each of these stages takes longer to heal and is more uncomfortable on a daily basis.
How to strengthen the shoulder joints?
The sports associated with a great strain on the shoulder belong mostly to the racket or throwing sports families: tennis, badminton, squash, soccer, baseball, track and field, discus sports, etc. These sports vary greatly in nature, but remain very technical, as the level of fine coordination of all the muscles involved is challenging, no matter what the movement required. Moderate practice of all these sports is a good way to strengthen this joint, but a special mention for swimming is in order as the movements in the water are performed against a constant resistance proportional to the force, which is ideal to avoid injuries.
You'll notice that I haven't offered any exercise tips this time around, but that's not for lack of trying. The problem is more that the exercises, whether they are to stretch, warm up or strengthen your muscles, are specific to your individual situation. The same exercise could be effective for one, useless for another or even harmful for a third individual. I therefore strongly encourage you to consult a health specialist who will be able to guide you, be it a kinesiologist or a manual therapist.
Izaak Lavarenne, NDG Physiotherapist
Izaak.laverenne@cliniquealtermed.com
NDG Clinic: (514) 664-3233
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -